
It starts with a promise that feels almost too clean.
A simple injection.
A natural solution.
Your own cells, repairing what’s been damaged.
The word “regenerative” lingers in the air, carrying weight it rarely defines.
But then the outcomes diverge.
One patient improves. Another plateaus. A third feels no change at all.
So what’s actually happening inside these treatments—and why doesn’t the story unfold the same way every time?
The answer isn’t in the syringe alone. It’s in the system the syringe enters.
Systems Explanation
Orthobiologics like PRP (platelet-rich plasma) and adipose-derived products, are often positioned as repair tools. But their real role is more subtle—and more dependent on context.
They interact with three primary systems:
• Inflammatory signaling
• Cellular communication pathways
• Tissue tolerance to mechanical load
These are not isolated processes. They are part of a dynamic network where timing, dosage, and environment matter.
What they can do:
• Modulate inflammatory cascades
• Deliver growth factors that influence signaling
• Support local biochemical environments
What they cannot do:
• Replace structurally damaged tissue
• Override poor biomechanics
• Compensate for inadequate rehabilitation
This distinction is where expectations often fracture.
Because while orthobiologics may influence biology, they do not control it.
Clinical Visualization
Imagine a joint as a living system under constant negotiation.
There is:
• Load coming in from movement
• Signals traveling between cells
• Sensitivity shaped by the nervous system
Now introduce PRP or adipose-derived material into that environment.
It doesn’t rebuild the structure like a construction crew.
It behaves more like a messenger—amplifying or redirecting communication already in progress.
If the system is:
• Overloaded → signals remain chaotic
• Underloaded → adaptation stalls
• Poorly coordinated → changes don’t integrate
The biologic input becomes just one voice in a crowded conversation.
And if the system isn’t prepared to receive it, the message doesn’t translate into meaningful change.
Clinical Insight 🧠
Orthobiologics may influence healing signals—but movement, load, and nervous system behavior determine whether those signals become lasting change.
This is why outcomes vary.
Not because the biology is inconsistent—but because the system it enters is.
PRP and adipose-derived orthobiologic products operate within specific regulatory boundaries.
They:
• Are autologous (sourced from the patient)
• Are minimally manipulated
• Are not FDA-approved drugs
• Are not classified as cures or guaranteed regenerative solutions
Their use is guided by:
• Clinical judgment
• Patient-specific variables
• Regulatory compliance
Not marketing language.
Understanding this framework is essential—not as a limitation, but as a recalibration of expectations.
Historical Perspective
In the 1990s, Arnold Caplan, PhD, a pioneer in mesenchymal stem cell research, introduced a concept that reshaped the field.
Initially believed to be direct tissue-building cells, these cells were later understood to function primarily as signaling and regulatory agents.
Caplan himself clarified this shift:
They don’t build tissue directly.
They coordinate the environment in which tissue behavior changes.
This distinction remains one of the most important—and most misunderstood—realities in orthobiologic care.
Long before biologics entered orthopedic care, recovery depended on:
• Load management
• Tissue adaptation
• Time-dependent healing
Orthobiologics did not replace these principles.
They entered the system as a potential modifier—not a substitute.
Clinical Context
When orthobiologics are considered, they are not used in isolation.
They are integrated into a broader clinical system that includes:
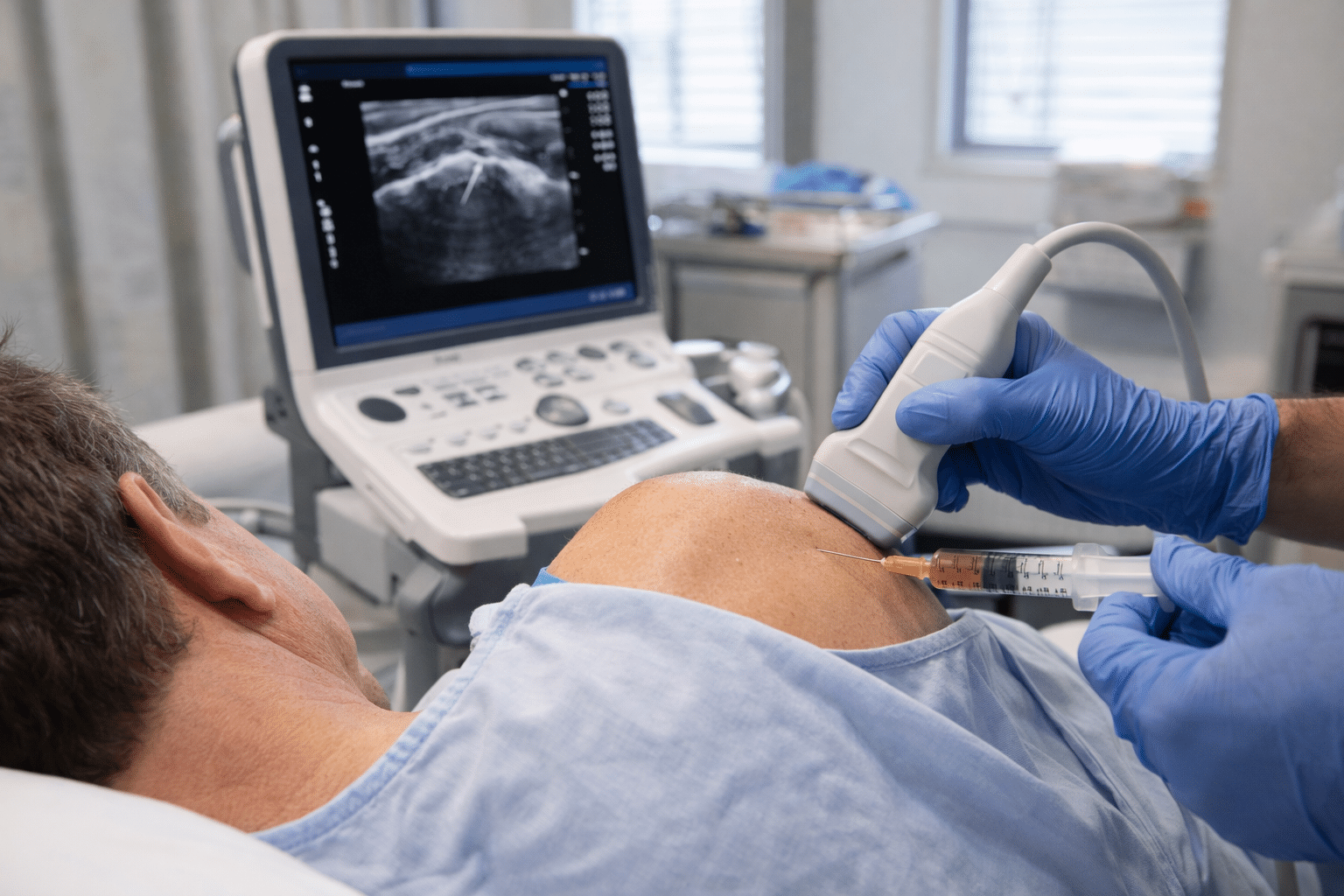
• Precise diagnosis
• Image-guided delivery (when appropriate)
• Structured rehabilitation planning
• Expectation alignment based on tissue behavior—not marketing outcomes
Their role is adjunctive.
Not primary.
Not standalone.
Not universally effective.
And most importantly—not interchangeable across patients or conditions.
E-E-A-T (Experience, Expertise, Authority, Trust)
Orthobiologic decision-making sits at the intersection of multiple domains:
• Musculoskeletal diagnosis
• Imaging interpretation
• Rehabilitation science
• Regulatory compliance
A biologic intervention without systems integration introduces variability.
A systems-based approach—where biology, movement, and load are aligned—creates a more stable clinical pathway.
Trust is not built on the intervention itself.
It’s built on how that intervention is positioned within the system.
Local Care, Global Science
In Northeast Indiana, patients often search for:
• “PRP for joint pain”
• “fat graft therapy explained”
• “regenerative medicine without surgery”
These searches reflect a growing awareness—but also a widening gap between expectation and clinical reality.
Bridging that gap requires clarity.
Not amplification.
Did You Know?
PRP contains a concentration of platelets that release signaling proteins—not structural tissue
Adipose-derived products include a mix of cells and signaling components, not isolated “stem cells” in the traditional sense
The term “regenerative medicine” is not a regulated clinical classification—it’s a descriptive label
FAQ
PRP introduces concentrated platelets that release signaling molecules, influencing inflammation and cellular communication—not rebuilding tissue directly.
Yes, adipose-derived treatments are a specific type of “stem cell therapy” or what we refer to as orthobiologics. While “stem cell therapy” is a broad term for treatments using undifferentiated cells to help ‘repair’ tissue, adipose-derived therapy specifically uses stem cells harvested from your own fat tissue
Outcomes depend on the interaction between the biologic input and the patient’s system—load, movement patterns, and tissue condition all play a role.
They may be considered in some cases as part of a broader strategy, but they do not replace structural interventions when those are required.
Yes. Rehabilitation determines how tissues adapt to load, which ultimately shapes long-term outcomes.
STAR Health Clinical Team
Focused on systems-based musculoskeletal care, integrating biologic therapies with rehabilitation, diagnostics, and long-term load management strategies.
Request an evaluation to determine whether biologic support is appropriate for your diagnosis.