
Orthobiologics, Regenerative Medicine, Biology, and Medical Reality—Without the Marketing
Did you ever notice how “stem cell therapy” seems to shift meaning depending on who is explaining it?
That inconsistency is not accidental. It reflects a gap between expectation and biological reality—a gap that continues to shape patient outcomes.
For many, regenerative medicine appears as a solution: restore tissue, eliminate pain, avoid surgery. But the truth unfolds more carefully. Modern regenerative medicine operates within strict biological limits, regulatory oversight, and system-dependent outcomes.
At STAR Health, this field is not positioned as replacement therapy. It is approached as orthobiologic support within a broader system of diagnosis, movement, and recovery.
🟦 SYSTEMS EXPLANATION
Regenerative medicine does not act independently. It functions inside a system already in motion.
Outcomes are shaped by how biologic inputs interact with:
• tissue integrity and baseline health
• mechanical load distribution
• neuromuscular signaling
• inflammatory regulation
• behavioral recovery patterns
When results vary, the biologic itself is rarely the sole variable.
The determining factor is whether the system receiving it is capable of responding.
A compromised joint under excessive load, or a nervous system amplifying pain signals, cannot be overridden by biology alone.
🟦 CLINICAL VISUALIZATION
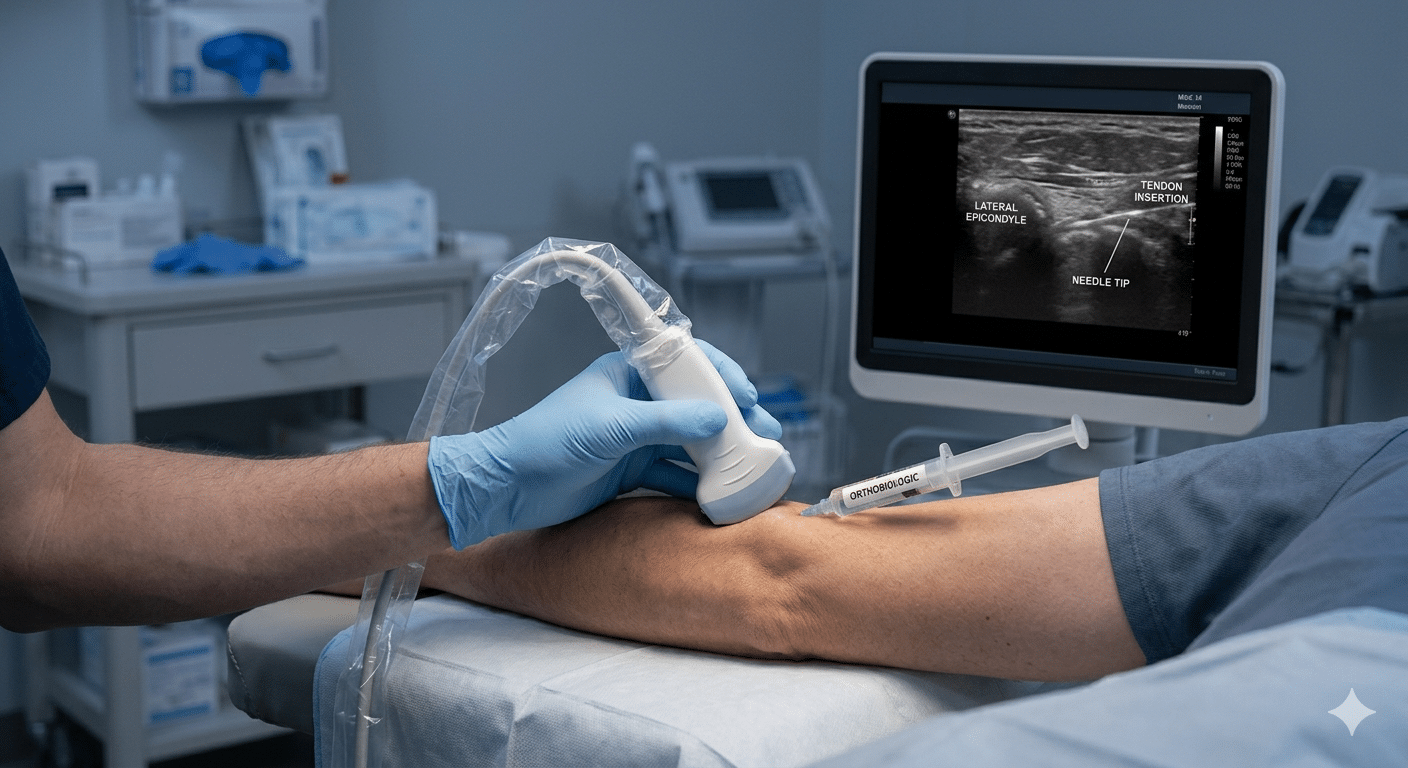
Imagine introducing a biologic concentrate into a joint.
At a microscopic level, the goal is not construction—but communication.
Cells do not “rebuild” structures in the way many assume. Instead, they release signaling factors that:
• influence inflammation
• modify cellular behavior
• support environmental conditions for repair
If the surrounding system is unstable—mechanically or neurologically—the signal is distorted.
The environment determines whether the message is received—or lost.
🟦 WHAT REGENERATIVE MEDICINE IS — AND IS NOT
What It Is
• a method using autologous biologics to influence tissue environments
• a way to modulate inflammation and cellular signaling
• an adjunct to structured rehabilitation and diagnosis
What It Is Not
• not guaranteed regeneration
• not equivalent to surgery
• not an FDA-approved drug therapy for orthopedic disease
• not universally appropriate
These distinctions are not limitations—they are safeguards.
🟦 FDA / CFR-COMPLIANT FRAMING
In U.S. musculoskeletal care, most regenerative approaches fall under orthobiologics, including:
• platelet-rich plasma (PRP)
• bone marrow–derived concentrates
• adipose-derived biologics
Regulatory realities define their use:
• they are not FDA-approved drugs
• they are minimally manipulated, patient-derived substances
• they are not marketed as cures
• they must be applied within clinical and ethical boundaries
Regulatory clarity protects both safety and expectation.
External reference: FDA Human Cells, Tissues, and Cellular Products Guidance
🟦 WHY OUTCOMES VARY
The most common question is simple: why do results differ?
The answers are less simple—and more important.
• Incorrect diagnosis
Treating the wrong structure cannot produce lasting change
• Mechanical overload
Ongoing stress disrupts any biologic support
• Nervous system amplification
Pain signaling may persist independent of tissue status
• Insufficient rehabilitation
Biology supports recovery, but movement retrains it
Regenerative medicine supports potential—it does not override physiology.
🟦 CLINICAL INSIGHT
Biologics influence the environment.
Rehabilitation determines adaptation.
Without alignment between the two, results plateau or regress.
🟦 E-E-A-T (EXPERIENCE / EXPERTISE / AUTHORITY / TRUST)
At STAR Health, regenerative medicine is integrated within a physician-guided framework that prioritizes:
• diagnostic precision
• regulatory compliance
• system-based care sequencing
Clinical decisions are not driven by trend or demand—but by biological appropriateness and patient-specific variables.
General authority: Mayo Clinic overview of regenerative medicine
🟦 HISTORICAL
Arnold Caplan — Case Western Reserve
The term “mesenchymal stem cell” originated with the expectation of tissue regeneration.
Over time, Caplan clarified a critical insight:
These cells function primarily as medicinal signaling cells, not direct builders of tissue.
This shift reframed the field—away from replacement, toward modulation.
🟦 LOCAL CARE, GLOBAL SCIENCE
In Northeast Indiana, patient searches often include:
• PRP for joint pain
• non-surgical recovery options
• regenerative medicine Fort Wayne
• stem cell therapy explained
Behind each search is the same need:
clear, accurate information without exaggeration.
🟦 FAQ
Does regenerative medicine regrow cartilage?
No. It may influence the joint environment, but full structural regeneration is not currently supported by evidence.
Is PRP the same as stem cell therapy?
No. PRP uses platelet-derived signaling factors, while stem-related therapies involve different biologic components and mechanisms.
Why do some people improve and others do not?
Outcomes depend on diagnosis, system readiness, mechanical factors, and rehabilitation—not just the biologic itself.
Is regenerative medicine safe?
When performed within regulatory guidelines using autologous materials, it is generally considered low risk—but not risk-free.
Can it replace surgery?
In some cases it may delay or reduce the need for surgery, but it is not a direct substitute.
🟦 DID YOU KNOW
Early regenerative medicine research assumed cells would rebuild damaged tissue directly.
Modern evidence shows their primary role is signaling—not construction.
Request an evaluation to determine whether biologic support aligns with your diagnosis and system-level recovery plan.
Contact us for an appointment today!